Abstracts
DDW Abstracts 2026
Addressing FIT Underutilization for CRC Screening in Asian Americans
Addressing Fecal Immunochemical Test Underutilization for Colorectal Cancer Screening in Asian Americans: Findings from a Patient-Centered Needs Assessment
Jeemin Kwon1, Selena Zhou1-2, Jessica J. Tuan4, Jennifer K. Bocek5, Jessica D. Calderon5, Sarah D. Meshkat5, Folasade P. May1-4
1UCLA Department of Internal Medicine, Los Angeles, CA, USA; 2Vatche and Tamar Manoukian Division of Digestive Diseases; UCLA David Geffen School of Medicine; 3Greater Los Angeles Veterans Affairs Health System, Los Angeles, CA, USA; 4UCLA Kaiser Permanente Center for Health Equity, Jonsson Comprehensive Cancer Center; 5UCLA Office of Population Health and Accountable Care
- Submission category: Health Services and Public Health Research; Health Care Delivery/Access/Quality OR Colorectal Neoplasia Screening; Non-Endoscopic
- Character limit: 2,900/2,900
Background: Colorectal cancer (CRC) screening rates are low among Asian Americans. In our medical center, a Mailed Fecal Immunochemical Test (FIT) Outreach Program was established in 2015 to increase screening participation, with only 16% uptake among Asian American patients. In this study, we aimed to identify the primary reasons why Asian American patients did not complete screening to inform future interventions.
Methods: The study setting is a large, urban academic health center with a defined primary care population and robust referral-based care. The Mailed FIT Outreach Program sends education, a FIT kit, and instructions in English to average-risk primary care patients overdue for CRC screening. Between 8/2024 and 1/2025, there were 334 Chinese, Japanese, or Korean patients who did not return a FIT. We contacted 201 (60.2%) via an electronic patient portal message (Epic MyChart), mailed letter, and/or phone call to complete a 12-item survey. Portal and mailed letters were in the patient’s documented preferred language; phone calls were conducted in English. We calculated frequencies and proportions for patient characteristics and survey item responses.
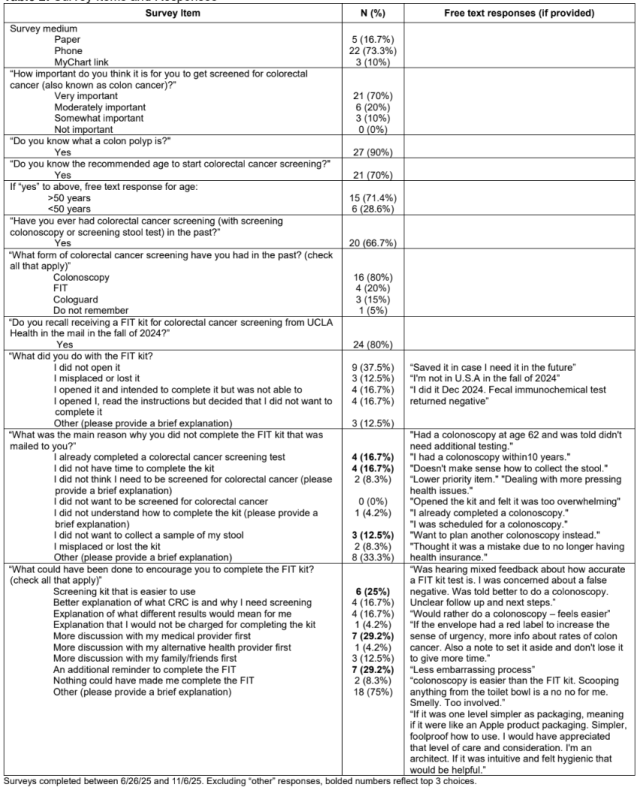
Results: The survey completion rate was 14.9% (30/201) (Table 1). The mean age of respondents was 57.5 years (sd=9.2), and 19 (63.3%) were female. Ten (33.3%) respondents were Chinese, 10 (33.3%) were Japanese, and 10 (33.3%) were Korean; 16 (53.3%) were born in the US. Twenty-one (70%) responded that CRC screening is “very important;” 21 (70%) reported knowing the age to start screening, of which 10 (47.6%) were correct; 27 (90%) reported knowing what a colon polyp is; and 20 (66.7%) reported prior screening (Table 2). Of those previously screened (20), colonoscopy was the most frequent method (16, 80%). Twenty-four (80%) recalled receiving the mailed FIT kit, of which 9 (37.5%) did not open the kit, 5 (20.8%) meant to complete the kit but did not, 4 (16.7%) did not want to complete the kit, and 3 (12.5%) misplaced the kit (Table 2). The most common reasons for not completing the kit were insufficient time (4,16.7%), felt up-to-date with screening (4,16.7%), and discomfort collecting stool (3,12.5%). The top three suggested ways to encourage FIT completion were an easier FIT kit (6, 25%), additional reminders (7, 29.2%), and more discussion with a medical provider (7, 29.2%). Respondents also provided free text responses indicating preference for colonoscopy and concerns about FIT accuracy (Table 2).
Conclusions: In this survey study of Asian American patients who did not complete a FIT, there was a mismatch between perceived importance of CRC screening and screening participation. Additional patient education on screening indications and FIT sensitivity, reminders, FIT kit redesign focused on user experience, or offering colonoscopy may increase participation in this patient demographic.
Table 1: Survey participant characteristics, n=30
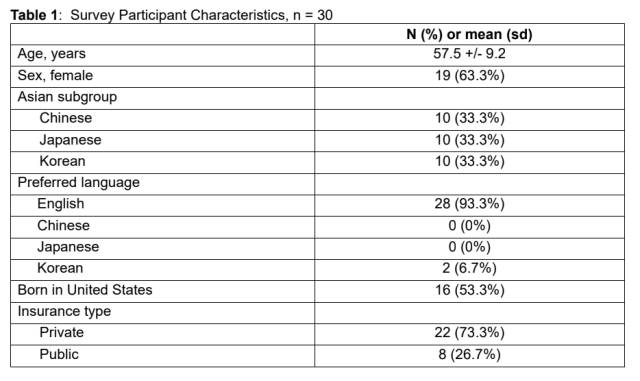
Table 2: Survey items and responses
Area Deprivation Index Predicts Colonoscopy After Abnormal FIT
Area Deprivation Index is a Predictor of Colonoscopic Follow-up After Abnormal FIT in a Large United States Health System
Yousif Arif, MD1-2; Alexandra Thomson, MD,MPH1-2; Jessica Tuan, MPH4, Jayraan Badiee, MPH1-2; Folasade P. May, MD, PhD, MPhil1-4
1Department of Medicine, David Geffen School of Medicine, UCLA Ronald Reagan Medical Center, University of California Los Angeles; 2Vatche and Tamar Manoukian Division of Digestive Diseases, Department of Medicine, David Geffen School of Medicine, University of California Los Angeles; 3Greater Los Angeles Veterans Affairs Healthcare System, Los Angeles, CA, USA; 4UCLA Kaiser Permanente Center for Health Equity, Jonsson Comprehensive Cancer Center
- Submission category: Colon; Clinical Science; Health Disparities
- Character count: 2876/2900 (including spaces)
Background: Patients with abnormal fecal immunochemical test (FIT) results require colonoscopic follow-up to complete colorectal cancer screening. Known predictors of follow-up include age, comorbidities, and health system practices (e.g., reminders, navigation). Less is known about how neighborhood-level deprivation may contribute. We aimed to evaluate the relationship between Area Deprivation Index (ADI), a validated composite measure for neighborhood-level disadvantage, and colonoscopic follow-up after abnormal FIT.
Methods: We conducted a retrospective cohort study in a large, multi-site academic health system in an urban setting. We included average-risk adults aged 45-75 with an abnormal FIT result between 7/1/2022 and 11/7/2024 and at least 12 months follow-up. The primary study outcome was colonoscopy completion within 6 months of abnormal FIT. Follow-up at 12 months was the secondary outcome. The primary independent variable was state-level ADI, a composite score derived from income, education, employment, and housing quality to provide a measure of a neighborhood's social and economic conditions. State ADI is categorized into deciles with the first decile (approx. ADI score 1-15) representing the least disadvantaged and the tenth decile (approx. ADI score 51-72) the most disadvantaged. Control variables included age, sex, race/ethnicity, and Elixhauser Comorbidity Index. We used descriptive statistics to summarize patient characteristics and performed multivariable logistic regression and Cox proportional hazards models to evaluate predictors of colonoscopic follow-up, with particular attention to the role of ADI.
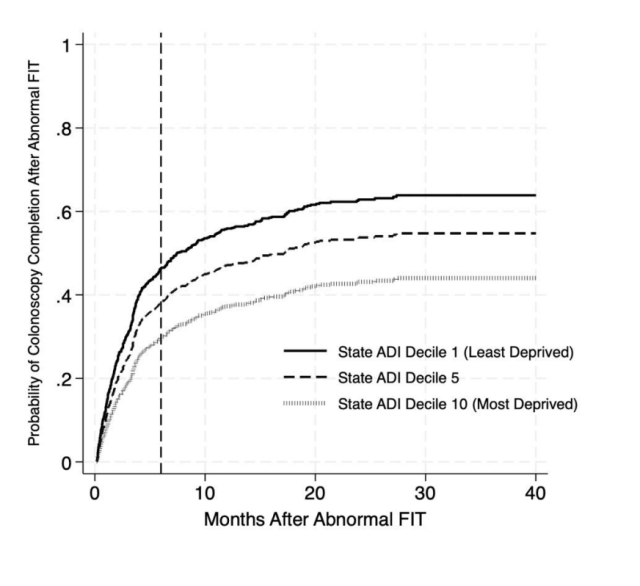
Results: We identified 1,083 patients with an abnormal FIT result during the study period. Mean age was 63 years (IQR 54-74); 53% were male, and 31.5% were non-Hispanic White (Table). The median ADI decile was 3. Overall, 547 patients (50.5%) completed colonoscopy by 6 months, and 625 (53.8%) did by 12 months. In adjusted logistic regression, higher ADI decile (aOR 0.89, 95% CI 0.82–0.97) was significantly associated with lower odds of colonoscopy completion at 6 months. This association remained significant at 12 months (aOR 0.91, 95% CI0.84-0.98). In the adjusted Cox proportional hazards model, higher state ADI was a significant predictor of lower likelihood of colonoscopy completion over time (aHR 0.94, 95% CI 0.89–0.99) (Figure).
Conclusion: In our large, academic, urban health center, high neighborhood deprivation was associated with lower odds of colonoscopic follow-up at 6 months, 12 months, and overall, for patients with an abnormal FIT result. ADI may serve as a practical risk stratification tool to identify patients at highest risk of being lost to follow up after an abnormal FIT result and can guide targeted, equity-focused interventions to address structural barriers to colonoscopic follow-up.
Table: Baseline characteristics of the study cohort by colonoscopy completion status.
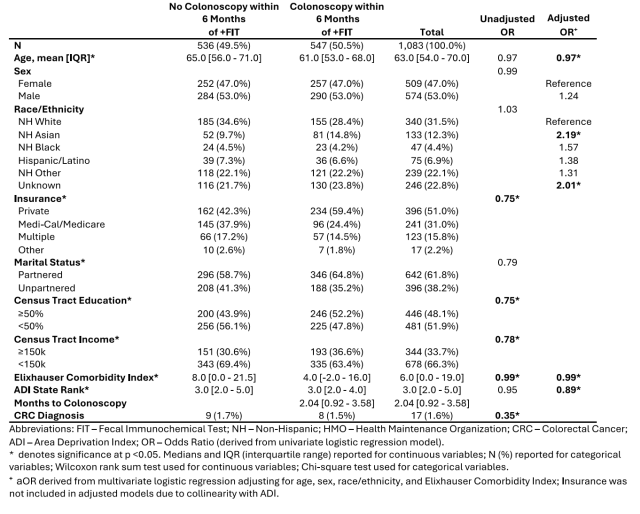
Figure: Adjusted probability of overall colonoscopy completion by state-level area deprivation index (ADI) deciles.
Colonoscopy Complications in Older Adults
Colonoscopy Complications in Older Adults: A Systematic Review and Meta-Analysis
Nicole P. Mirabadi, BA; Divya P. Prajapati, MD; Yi Le, MS; Alec Zadikian, BA; Lin Liu, PhD; Karen Heskett, MSI; Folasade P. May, MD, PhD, MPhil; Samir Gupta, MD, MSCS
- Proposed category: Colon; Clinical Science; Colorectal Neoplasia Surveillance; Endoscopic
Introduction: Risks of colonoscopy in older adults may inform decision-making surrounding colorectal cancer (CRC) screening and surveillance. We performed a systematic review and meta-analysis to characterize colonoscopy complications in older adults.
Methods: We searched PubMed, Web of Science, CINAHAL, and Embase through 11/2025 with keywords relevant to colonoscopy complications in older adults to identify studies with data reported for adults age >65; studies were excluded if data for patients with known CRC or disease states predisposing to CRC could not be disaggregated from patients without elevated CRC risk. Complication rates for adults aged ≥65 and ≥80 years were pooled for meta-analysis using random-effects models of proportions. Freeman–Tukey double arcsine transformation was applied to stabilize variance due to low event counts, and pooled estimates were expressed as rates per 10,000 colonoscopies with 95% confidence intervals (CI). A random effect model was also used for comparing complications for individuals age < 65 vs. > 65 years, and relative risk for complications was estimated.
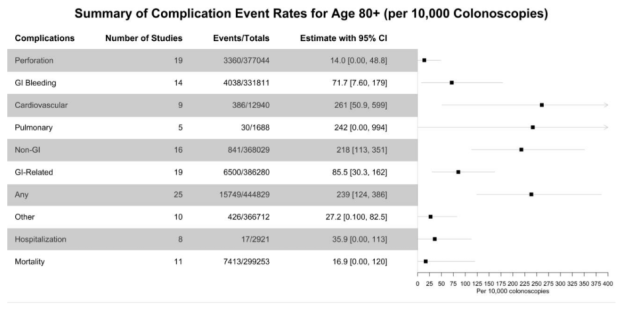
Results: Our search yielded 12,808 articles; 45 studies met inclusion criteria, and the number of studies included in meta-analysis of each outcome varied based on whether data specific to each outcome were reported (Figure 1). Mean reported age in studies of age ≥65 was 70.4 years with 47% female patients. Among adults age ≥65, the overall GI-related adverse event rate was 26.4/10,000 colonoscopies (95% CI: 10.2 – 48.8), with a perforation rate of 3.7/10,000 (95% CI: 0 – 11.7), and a GI bleeding rate of 26.3/10,000 (95% CI: 6.6 – 57.2; Figure 1). The overall non-GI adverse event rate was 133/10,000 (95% CI: 52.8 – 245). Mean reported age in studies of age ≥80 was 83.9 years with 61.3% female patients. Adults age ≥80 had an overall GI-related adverse event rate of 85.5/10,000 colonoscopies (95% CI: 30.3 – 162), perforation rate of 14/10,000 (95% CI: 0 – 48.8), GI bleeding rate of 71.7/10,000 (95% CI: 7.6 – 179), and overall non-GI adverse rate of 218/10,000 (95% CI: 113 – 351; Figure 2). Adults age ≥65 compared to <65 years had increased risk for GI-related adverse events (RR 2.0; 95% CI: 1.5 – 2.6), perforation (RR 2.6; 95% CI: 1.7 – 4.3) and GI bleeding (RR 1.8; 95% CI: 1.4 – 2.2); risk for non-GI adverse events approached significance (RR 1.55; 95% CI: 1.0 – 2.5).
Conclusion: Older adults are at increased risk of colonoscopy-associated complications compared to younger adults, with the highest rates observed among individuals age 80 and older. As the most comprehensive systematic review to-date of colonoscopy-associated complications in older adults, this analysis can inform patient-provider discussions as clinicians weigh benefits of CRC prevention against procedural risks in older adults.
Figure 1: Colonoscopy complications among patients age ≥65 years.
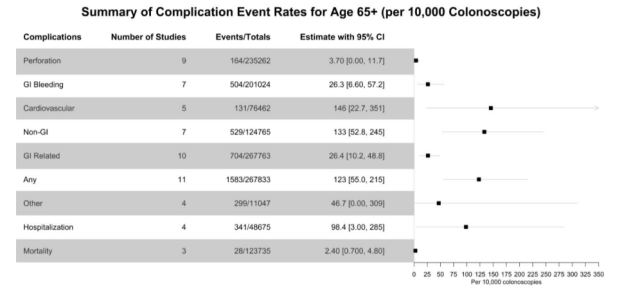
Figure 2: Colonoscopy complications among patients age ≥80 years.
Colorectal Cancer Outcomes Among Asian American Subgroups
Colorectal Cancer Outcomes Among Disaggregated Asian Subgroups: A 2006-2020 SEER Analysis
Matthew Y. Zhao, MD1 ([email protected]); Jayraan Badiee, MPH2 ([email protected]) Folasade P. May, MD, PhD, MPhil2-4 ([email protected])
1Department of Medicine, Icahn School of Medicine at Mount Sinai, New York, New York; 2Vatche and Tamar Manoukian Division of Digestive Diseases, Department of Medicine, David Geffen School of Medicine, UCLA, Los Angeles, CA, USA; 3Greater Los Angeles Veterans Affairs Healthcare System, Los Angeles, CA, USA; 4UCLA Kaiser Permanente Center for Health Equity, Jonsson Comprehensive Cancer Center, UCLA, Los Angeles, CA, USA
- Disclosures: None to report
- Character count: 2867/2900
- Abstract due: December 4, 2025; 9PM EST
- Abstract submission category: Colon; Clinical Science; Colorectal Cancer; Epidemiology and Diagnosis
Introduction: Despite varying colorectal cancer (CRC) outcomes across distinct Asian American subgroups, population-level analyses often assess Asian patients as a single aggregated category. We aimed to assess recent CRC outcomes among disaggregated Asian populations to better characterize subgroup-level heterogeneity.
Methods: Using National Cancer Institute (NCI) Surveillance, Epidemiology, and End Results (SEER) registry data from 2006 to 2020, we identified patients age ≥18 with a primary diagnosis of CRC. To assess outcomes among disaggregated Asian subgroups, we stratified patients into Chinese, Filipino, Japanese, Vietnamese, Korean, and Asian Indian/Pakistani. We also included a referent non-Hispanic (NH) White group. We identified predictors for regional or distant metastases at CRC diagnosis by multivariable logistic regression, as well as predictors for CRC-related mortality by multivariable Cox proportional hazards.
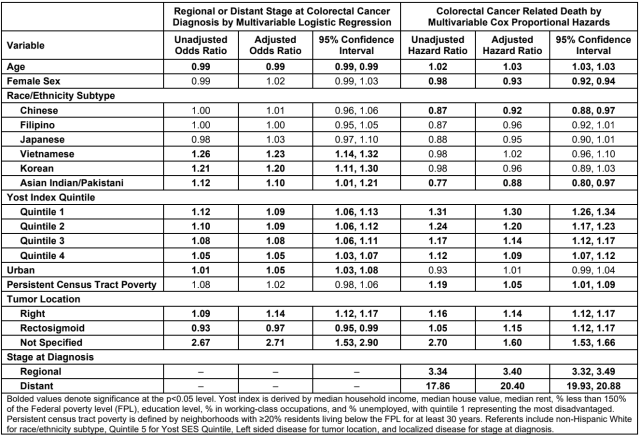
Results: Among 25,379 Asian patients, there were 6,585 (25.9%) Chinese, 6,399 (25.2%) Filipino, 4,309 (17.0%) Japanese, 3,047 (12.0%) Vietnamese, 2,964 (11.7%) Korean, and 2,075 (8.2%) Asian Indian/Pakistani patients included for analysis. We also included 234,948 NH White patients. Among all patients, median age was 66.0 (IQR 56.0-76.0), 53.0% were male, 59.2% had metastases at time of CRC diagnosis, and 27.9% suffered CRC-related mortality. Among disaggregated Asian subgroups, Vietnamese patients had the highest rates of metastasis at diagnosis (64.6%) and CRC-related mortality (28.2%) (Figure). In the multivariable logistic regression, Vietnamese (aOR 1.23, 95% CI 1.14,1.32), Korean (aOR 1.20, 95% CI 1.11,1.30), and Asian Indian/Pakistani (aOR 1.10, 95% CI 1.01,1.21) subgroups had increased odds of metastasis at time of diagnosis compared to NH White patients. Moreover, low socioeconomic status (SES) by Yost index quintile (YQ) was also associated with increased odds of metastatic disease (Table). In the multivariable Cox proportional hazards model, the Chinese (aHR 0.92, 95% CI 0.88,0.97) and Asian Indian/Pakistani (aHR 0.88, 95% CI 0.80,0.97) subgroups had decreased likelihood of mortality compared to NH White patients, whereas low SES and persistent census tract poverty predicted increased mortality risk (Table).
Conclusion: In this national cancer registry analysis, disaggregated Asian subgroups demonstrated heterogeneity in CRC outcomes. Vietnamese, Korean, and Asian Indian/Pakistani individuals had higher odds of presenting with metastatic disease, while Chinese and Asian Indian/Pakistani patients had lower mortality risk compared to White individuals with CRC. These findings highlight the importance of disaggregating Asian populations to accurately survey national CRC trends, identify groups at highest risk, and develop culturally relevant approaches to CRC prevention and management.
Figure: Survival curve by disaggregated Asian subgroup
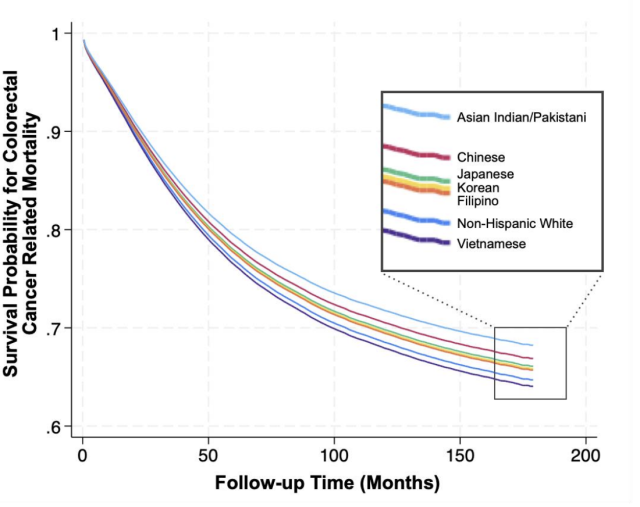
Table: Predictors of regional or distant stage at colorectal diagnosis by multivariable logistic regression and colorectal cancer related death by multivariable cox proportional hazards
Increasing Incidence of Early-Onset Gastric Carcinoma in the U.S.
Increasing Incidence of Early-Onset Gastric Carcinoma in the United States: A Population-Based SEER Analysis by Histologic Subtype
Sigrid S. Young, MD1 ([email protected]); Jayraan Badiee, MPH1 ([email protected]); Folasade P. May, MD, PhD, MPhil1-3 ([email protected])
1Vatche and Tamar Manoukian Division of Digestive Diseases, Department of Medicine, David Geffen School of Medicine, UCLA, Los Angeles, CA, USA; 2Greater Los Angeles Veterans Affairs Healthcare System, Los Angeles, CA, USA; 3UCLA Kaiser Permanente Center for Health Equity, Jonsson Comprehensive Cancer Center, UCLA, Los Angeles, CA, USA
- Limit: 2,880/2900 characters including spaces
- Submission deadline: December 4, 2026; 6PM PST, 9PM EST
- Presentation type: Oral or poster
- Abstract track: Stomach & duodenum
- Category: Gastric Pre-Neoplastic and Neoplastic Conditions; Epidemiology and Diagnosis
Background: Gastric cancer (GC) is the fifth most common cancer and the fourth leading cause of cancer-related deaths worldwide. In the United States, routine endoscopic screening is not recommended for average-risk individuals, and most patients present with advanced disease. Prognosis varies substantially by histology, with 5-year survival of 36% for gastric adenocarcinoma (GA) versus 81% for gastric neuroendocrine tumors (GNET). Given rising gastrointestinal cancer rates in young adults, we aimed to evaluate temporal trends in GC incidence by histologic subtype and age.
Methods: We analyzed 2004–2022 data from the National Cancer Institute’s Surveillance, Epidemiology, and End Results (SEER) registry. We included patients (1) aged ≥15 years, (2) diagnosed with a primary gastric malignancy, (3) with histologically confirmed GA, GNET, signet ring cell carcinoma (SRCC), or other invasive carcinoma, and (4) no concurrent or prior cancer diagnoses. Age-standardized incidence rates (ASIR) and annual percentage change (APC) were calculated and stratified by age group (15–49 vs. ≥50 years) and GC subtype. Joinpoint regression was used to assess trends and statistical significance.
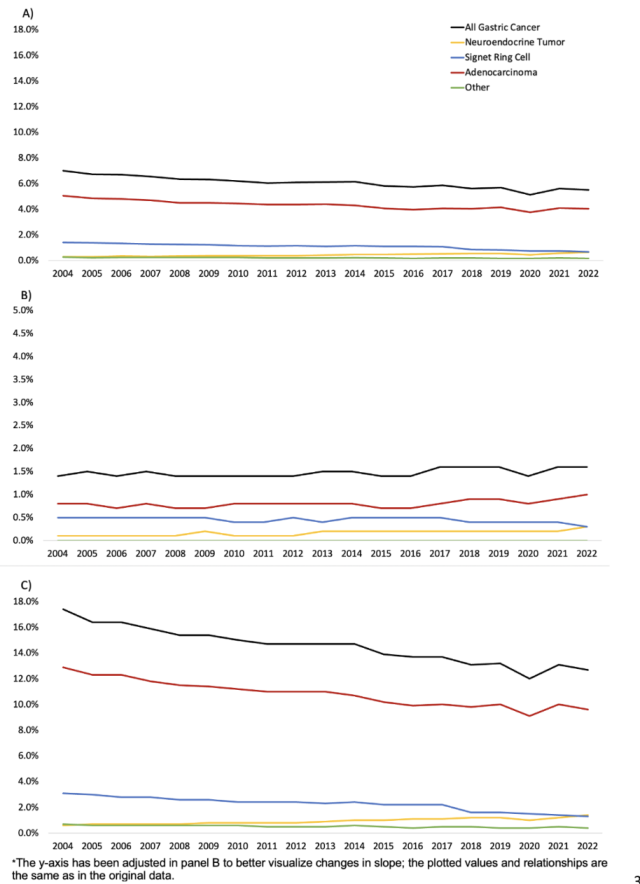
Results: There were 137,641 people with GC (62% male; median age 66.0 [IQR 56.0–76.0]; 86.5% ≥50 years). Most had GA (71.7%), followed by SRCC (17.7%), GNET (7.3%), and other invasive carcinoma (3.4%). Overall, 49.8% were non-Hispanic White, 23.6% Hispanic, 13.4% non-Hispanic Black, 12.5% non-Hispanic Asian/Pacific Islander, and 0.7% non-Hispanic American Indian/Alaska Native. For all ages combined, incidence declined for GC, GA, SRCC, and other gastric carcinoma (APC −1.30, p<0.001; APC −1.30, p<0.001; APC −2.0, p=0.03; APC −15.8, p=0.004), while it increased for GNET (APC 3.90, p<0.001). GA incidence decreased in people age ≥50 years (APC −1.56, p<0.0001) but increased for people age <50 (APC +1.01, p=0.03). Overall GC incidence declined in patients age ≥50 (APC −1.67, p<0.0001) but rose modestly in those age <50 (APC +0.60, p=0.057). In both age cohorts, SRCC incidence declined, while GNET incidence increased over time (Table, Figure).
Conclusion: Despite overall declines in GC incidence and sustained decreases among people age ≥50 years, incidence is rising in people under age 50, driven primarily by increasing GA2 incidence in this younger cohort. GNET incidence has also increased across all ages since 2004. These age- and histology-specific shifts demonstrate that the emerging burden of early-onset gastrointestinal cancers includes GC and is not uniform across subtypes. The growing incidence of GA in younger adults, in contrast to declines in older populations, suggests an evolving epidemiologic pattern. Further research is needed to identify the drivers underlying these selective increases in order to address the growing burden of early-onset disease.
Table: Annual percentage change (APC) in gastric cancer incidence by gastric cancer subtype and age cohort
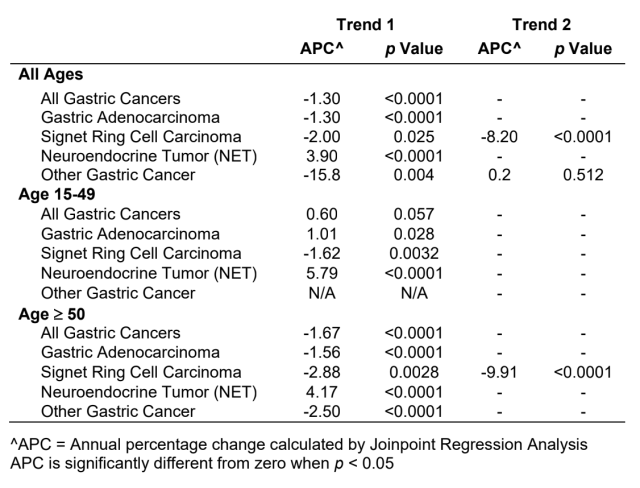
Figure: Age-standardized incidence rate over time by gastric cancer subtype for a) all patients (n=137,641); b) people age 15-49 (n=18,527); and c) people age 50 and older (n=119,114)
Minimal Improvements in Colorectal Cancer Screening in U.S. FQHCs
A Decade of Massive Patient Population Growth but Minimal Improvements in Colorectal Cancer Screening Participation in United States Federally Qualified Health Centers from 2014 to 2024
Megan R.M. Aaronson, MD, MS1 ([email protected]); Matthew Y. Zhao, MD2 ([email protected]); Jayraan Badiee, MPH3 ([email protected]) Folasade P. May, MD, PhD, MPhil3-5 ([email protected])
1Department of Medicine, David Geffen School of Medicine, UCLA, Los Angeles, CA, USA; 2Department of Medicine, Icahn School of Medicine at Mount Sinai, New York, New York; 3Vatche and Tamar Manoukian Division of Digestive Diseases, Department of Medicine, David Geffen School of Medicine, UCLA, Los Angeles, CA, USA; 4Greater Los Angeles Veterans Affairs Healthcare System, Los Angeles, CA, USA; 5UCLA Kaiser Permanente Center for Health Equity, Jonsson Comprehensive Cancer Center, UCLA, Los Angeles, CA, USA
- Disclosures: None to report
- Character count: 2873/2900
- Abstract due: December 4, 2025; 9PM EST
- Submission category: Colon; Clinical Science; Health Disparities
Introduction: United States (US) Federally Qualified Health Centers (FQHCs) provide primary care services, including colorectal cancer (CRC) screening, for millions of Americans regardless of their ability to pay. Populations served in these settings have suboptimal CRC screening rates and outcomes. We aimed to evaluate 10-year trends in FQHC characteristics and CRC screening participation.
Methods: We used the Uniform Data System (UDS), the only source for national FQHC quality data, to perform cross-sectional analyses of CRC screening rates for all US FQHCs. We abstracted CRC screening rates for each FQHC from 2014 to 2024 and FQHC characteristics in the years 2014 and 2024, including the percentage of patients who were: age 45-74, uninsured, non-English speaking, >200% of the federal poverty level (FPL), and experiencing homelessness. We grouped FQHCs by majority race/ethnicity served (non-Hispanic [NH] White, NH Black, Hispanic/Latino, NH Asian, NH Other), urban/rural status, and US region (West, South, Midwest, Northeast). We used paired Wilcoxon signed-rank tests to compare FQHC characteristics and screening rates for all FQHCs in 2014 and 2024. We also calculated percent change in FQHC characteristics from 2014 to 2024 and performed linear regression to evaluate the relationship between FQHC characteristics and change in CRC screening participation over time.
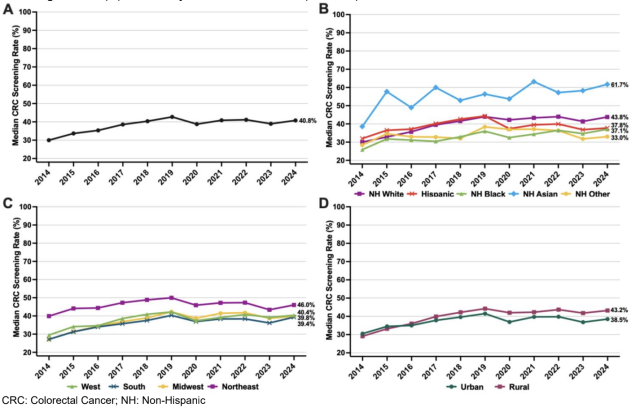
Results: There were 7,430,162 patients eligible for CRC screening at 1,271 US FQHCs in 2024, compared to 3,936,450 patients in 1,192 FQHCs in 2014 (Table). FQHC patient-mix characteristics changed significantly from 2014 to 2024 (Table). The median CRC screening rate for all FQHCs was 30.0% in 2014 and 40.8% in 2024 (Figure 1A). Screening participation increased from 2014 to 2024 regardless of the majority race/ethnicity served, US region, and urban/rural status (Figure 1B, 1C & 1D). In our adjusted model, FQHCs in states that adopted Medicaid expansion (coef 4.05, 95% 1.02 - 7.08) and FQHCs with a greater percentage of patients with income >200% FPL (coef 0.16, 95% CI 0.02 - 0.30) experienced a significant increase in CRC screening participation from 2014 to 2024. Conversely, FQHCs with a high percentage of uninsured patients (coef -0.22, 95% CI -0.37 - -0.08) saw a significant decrease in screening participation over time (data not shown).
Discussion: The number of age-eligible patients served by FQHCs nearly doubled from 2014 to 2024, and FQHCs became more diverse. Despite this population growth, gains in CRC screening participation have slowed and remain 2 below pre–COVID-19 levels. Our findings suggest that structural factors, including Medicaid expansion status and socioeconomic composition, impact a FQHC’s capacity to screen patients. Sustained policy support for FQHCs is essential to advance progress and ensure equitable CRC screening on a national scale.
Table: Characteristics of United States federally qualified health centers in 2014 and 2024
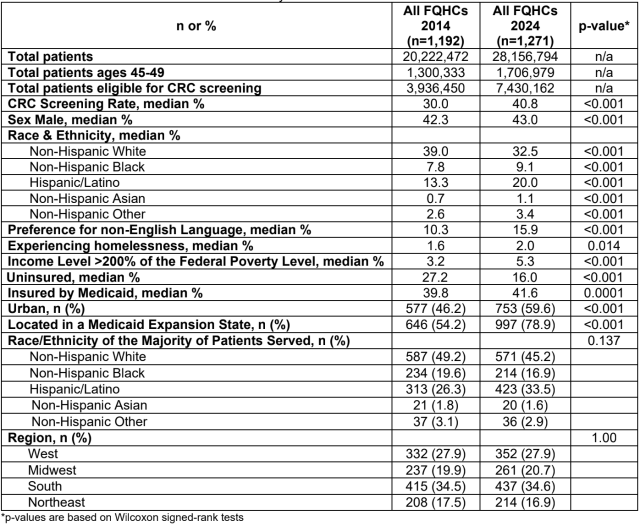
Figure 1: Trends in median colorectal cancer screening rates from 2014-2024 for (A) All U.S. FQHCs; (B) FAHCs by race/ethnicity of majority of patients served; (C) FQHCs by U.S. region; and (D) FQHCs by urban/rural status; (n=1,271)
Population Outreach with Decision Aid Increases Colorectal Screening
Population Health Outreach with a Shared Decision Aid Increases Uptake of Colorectal Cancer Screening for Average-Risk Adults
Thomson, Alexandra E., MD, MPH1-2, Tuan, Jessica J., MPH3, Fujimoto, Jeffrey MD, MBA1, Smith, Laurie N., MPH4, Badiee, Jayraan, MPH2, May, Folasade P., MD, PhD, MPhil1,2,3,5
1Department of Medicine, David Geffen School of Medicine, UCLA, Los Angeles, CA, USA; 2Vatche and Tamar Manoukian Division of Digestive Diseases, Department of Medicine, David Geffen School of Medicine, UCLA, Los Angeles, CA, USA; 3UCLA Kaiser Permanente Center for Health Equity, Jonsson Comprehensive Cancer Center, UCLA, Los Angeles, CA, USA; 4WiserCare, Los Angeles, CA, USA; 5Greater Los Angeles Veterans Affairs Healthcare System, Los Angeles, CA, USA
- Disclosures: None to report
- Funding: Institutional, Melvin and Bren Simon Digestive Diseases Center
- Submission category: Practice management: clinical science: Performance Metrics, Process Improvement, Quality Improvement and Implementation
- Character count: 2895/2900
Introduction: Population health outreach can increase colorectal cancer (CRC) screening participation within health systems. The WiserCare (WC) CRC screening module is an electronic shared decision aid that facilitates patient-provider discussions about CRC screening test options to promote screening participation. We evaluated the impact of the module on screening uptake in a large United States health system.
Methods: The study setting is an urban, tertiary care health system with over 300 primary care providers, 67 clinics, and 5 endoscopy sites. In 2/2023, the health system launched My Action Plan (MAP), an EHR-based population health outreach program that sends electronic education and shared decision aids to patients overdue for preventive care measures. For primary care patients overdue for CRC screening, MAP sends the WC CRC screening module, which helps patients select a screening modality that meets their risk profile and personal preferences (fecal immunochemical test [FIT], colonoscopy, CT colonography, sigmoidoscopy, or stool DNA). Patients who remain unscreened are mailed a FIT. For this evaluation, we included primary care patients age 45 to 75 at average-risk for CRC and overdue for screening between 2/1/2023 and 7/31/2024. The primary outcome was CRC screening participation at 9 months (any modality), We compared screening rates for patients who (1) completed the WC module (group 1), (2) did not access the WC module (group 2), and (3) accessed but did not complete the WC module (group 3). We used Kruskal Wallis, chi-square tests, and pairwise comparisons to summarize patient characteristics and compare screening completion in the 3 groups.
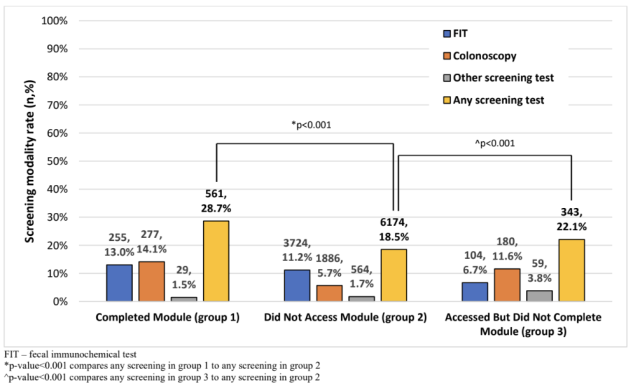
Results: Among the 36,856 patients sent the WC module during the study period, median age was 54.1 years (IQR 49.1-62.1), 54% were female, and 49% were non-Hispanic White (Table). Overall, 9.5% accessed the module. Of patients who completed the module (n=1,958), 56% were female, 54% were non-Hispanic White, and 79% were privately insured (Table). Screening participation in group 1 was 28.7%, compared to 18.5% in group 2 and 22.2% in group 3 (all pairwise p<0.001). For group 1 and group 3, colonoscopy was most common (49.4% and 52.5%, respectively), followed by FIT (45.5% and 30.3%, respectively). For group 2 patients, FIT (60.3%) was followed by colonoscopy (30.5%) (Figure).
Conclusions: In this population health outreach program, engagement with the shared decision aid was low, but screening participation was significantly higher among patients who at least accessed the module. Patients who accessed the module were more likely to complete colonoscopy than FIT. The findings support that population outreach through shared decision aids can increase CRC screening participation independent of clinical visits, offloading primary care providers and increasing health system quality performance metrics.
Table: Patient characteristics and study outcomes by CRC screening module completion status; N=36,856
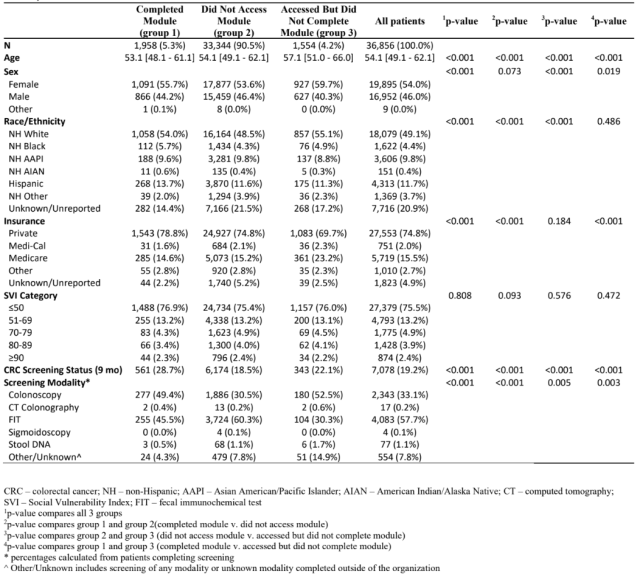
Figure: Screening participation and modalities chosen for each study group and overall at 9 months; n=7,078
Provider Perspectives on CRC Surveillance Among Veterans Age 75+
Provider Perspectives on Colorectal Cancer Surveillance Among Veterans Age 75 and Older: The SurvOlderAdults (Surveillance Colonoscopy in Older Adults) Study
Neetu Chawla, PhD; Tamra Burns Loeb, PhD; Samir Gupta, MD; Lin Liu, PhD; Joshua B Demb, PhD; Jiyue Qin, MS; Ashley Earles, MPH; Mark Lamm; Benjamin J Seligman, MD, PhD; Folasade P May, MD, PhD, MPhil
- Characters: 2858 (limit 2900)
Background: Older adults (age75) and their providers face challenging decisions regarding whether to continue or forgo post-polypectomy colonoscopic surveillance, given the need to balance cancer detection and prevention with procedure risks and competing healthcare priorities. We conducted qualitative interviews with providers in the Veterans Health Administration (VA) to assess perspectives on surveillance decision-making for older adults.
Methods: We conducted 24 semi-structured interviews with primary care providers (PCPs), gastroenterologists (GIs), and geriatricians from two VA sites after reaching out to 90 total providers (26.7% response). Interviews were structured using domains from a multi-level framework modelled after the Socio-Ecological framework, including factors at the patient-, provider-, system-, and policy-levels. We used a rapid analysis approach to identify themes according to the multi-level framework.
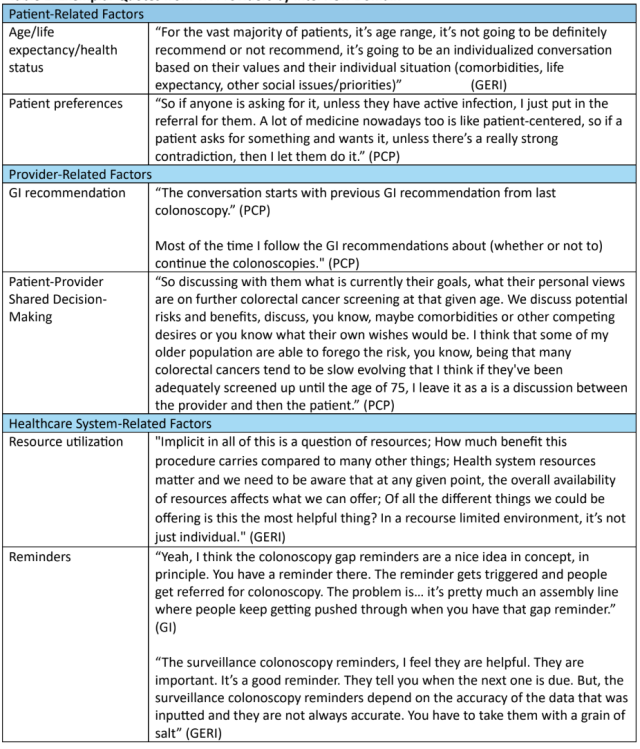
Results: Our sample included 12 PCPs, 8 GIs, and 4 Geriatricians. Providers discussed the following patient-level factors when considering surveillance for older adults: age, life expectancy, health status/comorbidities, patient preferences, and identifying the highest priority for patients’ overall health needs. Key provider-level themes were that: many follow GI provider recommendations; some factor in whether patients would pursue treatment if tumors were found through surveillance; some heavily discuss patient preferences and make decisions based upon individual circumstances; and differences existed in attitudes towards whether to continue surveillance based on provider type, with geriatricians being more likely to note that some 75 year olds “can run a marathon” while others are “bed bound.” Providers also brought up factors related to the healthcare system, such as the use of reminders, with some finding them “helpful” and others noting they are “good in principle but have their limitations.” Providers had differing impressions about continuing surveillance colonoscopies for older patients within VA, with some noting “poor resource utilization” and needing “a way to screen patients to see if they are appropriate or not,” while others said that continuation was “the status quo” but it would “be nice to define who does not need it based on individual risk.”
Conclusions: VA providers identified several factors at the patient-, provider-, and health system-levels that influence surveillance colonoscopy decision-making for older adults in the VA. We identified notable differences in perspectives about the importance of patient age, reliance on GI recommendations, and resource utilization for continuing surveillance. Future research should assess patient-level attitudes towards CRC surveillance in older adults to understand the alignment between provider and patient perspectives.
Figure 1: Adapted version of Steve Taplin's multi-level framework for CRC surveillance among older Veterans
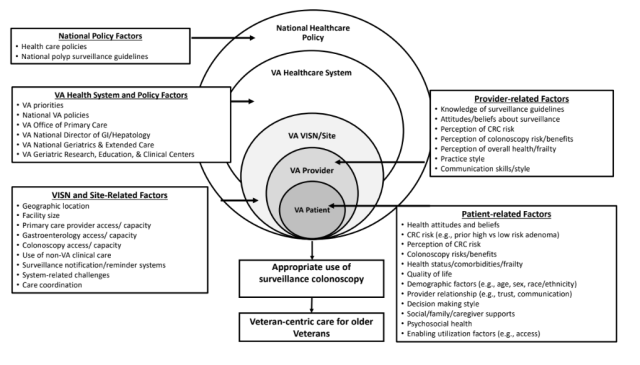
Table 1: Exemplar quotes from VA providers by interview domain
Root-Cause Analysis of Post-Endoscopy Esophageal Neoplasia at the VA
Root-Cause Analysis of Post-Endoscopy Esophageal Neoplasia at the Veterans Health Administration
Zainab Aziz; Rahul Karna; Mohammad Bilal; Mei Leng; Anders Westanmo ([email protected]); Jason A. Dominitz; Samir Gupta; Folasade May; David Katzka; Nicholas J. Shaheen; Sachin Wani; Jennifer M. Kolb
Background: Surveillance endoscopy is recommended in Barrett’s esophagus (BE) for early neoplasia detection; however current practices have not diminished death from esophageal adenocarcinoma (EAC). Post-endoscopy esophageal neoplasia (PEEN), defined as high-grade dysplasia (HGD) or EAC detected after an apparently negative exam and before the next appropriate surveillance interval, may indicate suboptimal surveillance or missed lesions. The specific contributors to PEEN are not well described.
Methods: We conducted a root-cause analysis to identify drivers of PEEN in a national cohort of BE patients from the Veterans Health Administration between 2010-2024. Veterans with an index endoscopy of non-dysplastic BE or indefinite for dysplasia and a subsequent diagnosis of HGD or EAC between 6 months to 3 years later were included. A panel of three BE experts reviewed primary source records and independently rated examination quality and follow-up recommendations (Figure). Index endoscopy was deemed adequate according to the following criteria 1) appropriate landmark identification, 2) use of virtual chromoendoscopy, and 3) use of Seattle biopsy protocol. A more lenient definition of adequacy excluded chromoendoscopy.
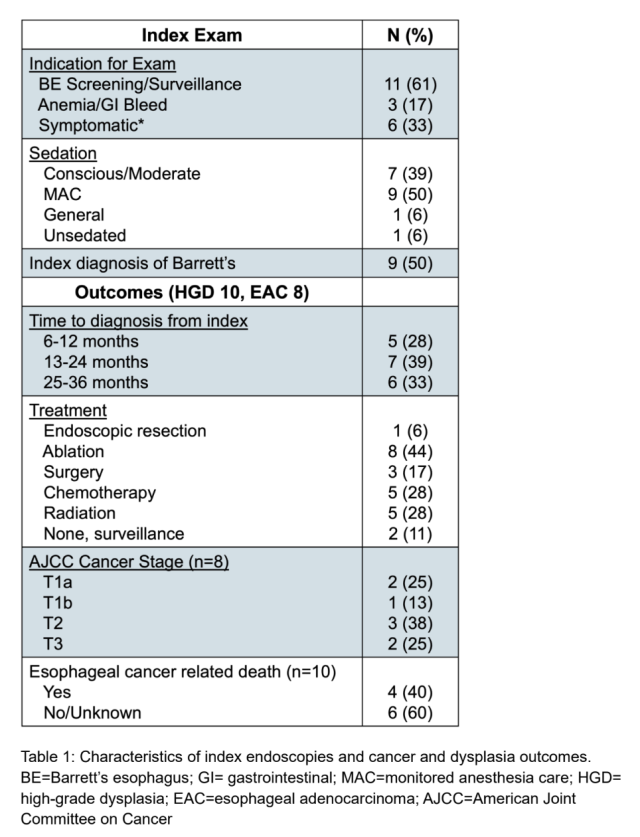
Results: 18 PEEN cases were identified (10 HGD, 8 EAC) with a mean time to diagnosis of 1.6 years (Table). 5 of the cancers were advanced stage T2/T3 and required chemotherapy and radiation. On index endoscopy, landmarks were appropriately identified in 59% of cases, chromoendoscopy use was documented infrequently (17%) and Seattle protocol biopsy was used less than half the time (44%). In 3 of the 18 cases a visible lesion was identified- 1 had inadequate sampling, and 2 had adequate sampling with possible causes for PEEN as inappropriate follow-up or possible additional missed lesion. For the remaining 15 cases without a visible lesion, the majority had inadequate endoscopy (14, 78%) with a possible explanation being a missed lesion. There was one case with panel disagreement over adequacy of exam; inappropriate follow-up was the likely cause of PEEN. Using less stringent criteria (landmarks + Seattle), 10 cases (56%) were determined to have inadequate examination, 1 adequate (6%), and there was disagreement over adequacy for the other 4 cases (22%).
Conclusion: Among a national cohort of Veterans with BE, root-cause analysis with expert panel adjudication of PEEN cases demonstrated suboptimal quality of endoscopic examination. Inadequate description of BE landmarks, with no demarcation of length or Prague classification and hiatal hernia, and limited use of the Seattle protocol and chromoendoscopy may have resulted in missed lesions. These results can inform intervention strategies, including use of standardized reporting systems, tissue sampling protocols, and optimized technology for neoplasia detection.
Figure 1: Root-cause analysis workflow for expert panel. While there may be other causes of PEEN following an adequate endoscopy (such as possible missed lesion or inadequate pathology read), in our cohort there was only one case, with inappropriate follow up recommended. PEEN=post-endoscopy esophageal neoplasia; HDG=high-grade dysplasia; EAC=esophageal adenocarcinoma.
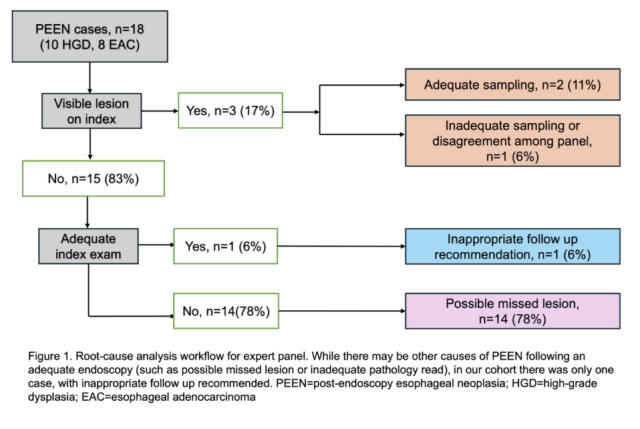
Table 1: Characteristics of index endoscopies and cancer and dysplasia outcomes. BE=Barrett’s esophagus; GI= gastrointestinal; MAC=monitored anesthesia care; HGD= high-grade dysplasia; EAC=esophageal adenocarcinoma; AJCC=American Joint Committee on Cancer
DDW Abstracts 2025
Association of clinical and demographics variables and incident cirrhosis by FIB-4 score in a large primary care cohort
Carrie R. Wong, MD, PhD; Analissa Avila, MS; Yvonne N. Flores, PhD; Folasade P. May, MD, PhD, MPhil; Beth Glenn, PhD; Roshan Bastani, PhD
Introduction: The Fibrosis-4 (FIB-4) score is widely used to stratify risk of advanced fibrosis and is most appropriately used in low-prevalence primary care settings. The FIB-4 score can be reassessed within 3 years depending on the patient’s metabolic risk factors. However, recent studies have suggested limitations in FIB-4 score accuracy even in nonspecialty settings. We aimed to identify the association of clinicodemographic variables and risk of incident cirrhosis by FIB-4 score in a large primary care cohort. Click here for full abstract
Colorectal cancer screening rates at Federally Qualified Health Centers serving majority LGBTQIA+ patients
Vidhi Singh, BS; Matthew Y. Zhou, MD; Helen Xu, MD; Megan R.M. Aaronson, MD, MS; Jayraan Badiee, MPH; Folasade P. May, MD, PhD, MPhil
Introduction: LGBTQIA+ adults in the United States (US) often face unique barriers to health care services that are augmented by intersecting marginalized identities. LGBTQIA+ patients receiving preventive services at Federally Qualified Health Centers (FQHCs) represent a particularly underserved and understudied population. We assessed colorectal cancer (CRC) screening rates and predictors of screening in US FQHCs serving primarily LGBTQIA+ adults compared to FQHCs serving primarily cisgender-heterosexual (cishet) adults. Click here for full abstract
Comparing the effectiveness of two mailed outreach interventions to increase colorectal cancer screening in community health centers
Folasade P. May, MD, PhD, MPhil; Jessica J. Tuan, MPH; Suzanne Brodney, PhD, MS; Beth Glenn, PhD; Yixuan Zhou; Adjoa Anyane-Yeboa, MD, MPH; Nicolette J. Rodriguez, MD, MPH; Caylin Marotta, MPH; Susan Regan, PhD; Sapna Syngal, MD, MPH; Andrew T. Chan, MD, MPH; Catherine Jeffries; Kelley Le Beaux, MA; Samantha Kuney, MA; Kimberly Schoolcraft; Anjelica Q. Davis, MPPA; Chinedu Ukaegbu, MBBS, MPH; Erica T. Warner, ScD, MPH; Beverly Moy, MD, MPH; David A. Drew, PhD; Gina Johnson; Yuchiao Chang, PhD; Jennifer S. Haas, MD, MSc
Introduction: Community health centers (CHCs) in the United States (US) provide primary care services to over 31 million low-income and uninsured individuals. In CHCs, stool-based colorectal cancer (CRC) screening modalities are common; however, screening rates and colonoscopic follow-up after abnormal screening are below the national average. This 2-arm pragmatic trial aims to increase CRC screening and follow-up after abnormal screening in CHCs in 2 US regions. Click here for full abstract
Current state analysis of disease monitoring practices after initiation of advanced therapies in patients with inflammatory bowel disease
Bita Shahrvini, MD; Andrew Chang, MD; Alexandra C. Greb, MD; Mark Baniqued, MD; Divya Prajapati; Rhett Harmon, MD; Nirupama Bonthala, MD; Jenny S. Sauk, MD; Gaurav Syal, MD, MSHS; Folasade (Fola) Popoola May, MD, PhD, MPhil; Berkeley N. Limketkai, MD, PhD
Introduction: Advanced therapies (AT) are effective for inducing remission in inflammatory bowel disease (IBD). A treat-to-target (T2T) approach with close monitoring of symptoms and inflammation is crucial to optimize outcomes. This study investigates the current state of T2T monitoring practices after AT initiation and risk factors for suboptimal monitoring for IBD patients at a large tertiary care center. Click here for full abstract
Current state analysis of malnutrition screening for patients with inflammatory bowel disease reveals telehealth is a risk factor for lack of screening
Bita Shahrvini, MD; Andrew Chang, MD; Alexandra C. Greb, MD; Mark Baniqued, MD; Divya Prajapati; Rhett Harmon, MD; Christina Fasulo, MS, RDN, CNSC; Nirupama Bonthala, MD; Jenny S. Sauk, MD; Gaurav Syal, MD, MSHS; Folasade (Fola) Popoola May, MD, PhD, MPhil; Berkeley N. Limketkai, MD, PhD
Introduction: Patients with inflammatory bowel disease (IBD) have an increased risk of malnutrition. The prevalence of malnutrition is up to 50% among ambulatory IBD patients and has been associated with worse outcomes, prompting recommendations for regular malnutrition risk screening in all IBD patients. This quality improvement (QI) study details a current state analysis of outpatient gastroenterology (GI) malnutrition screening practices for IBD patients at a large, tertiary care center and evaluates risk factors for lack of malnutrition screening. Click here for full abstract
Disaggregation of race and ethnicity data to examine colorectal cancer screening rates at Federally Qualified Health Centers
Matthew Y. Zhao, MD; Helen Xu, MD; Vidhi Singh, BS; Megan R.M. Aaronson, MD, MS; Jayraan Badiee, MPH; Folasade P. May, MD, PhD, MPhil
Introduction: Assessing disaggregated race and ethnicity data for colorectal cancer (CRC) screening is critical for recognizing and equitably addressing health disparities. However, many data sources lack the granularity necessary to do so. The Uniform Data System (UDS) reports annual quality data for all United States (US) Federally Qualified Health Centers (FQHCs), and for the first time now includes disaggregated data for Hispanic/Latino and Asian demographic groups. To better contextualize CRC screening disparities at FQHCs, we evaluated FQHC CRC screening rates using this disaggregated data. Click here for full abstract
Documentation practices of surveillance colonoscopy interval recommendations following screening colonoscopy in a large academic health center
Robert Tamai, MD; Folasade P. May, MD, PhD, MPhil
Introduction: Gastroenterologists routinely provide surveillance colonoscopy interval recommendations based on endoscopic and pathologic findings and 2020 Multi-Society Task Force (MSTF) guidelines. Documentation of these recommendations is critical so that patients undergo the appropriate surveillance to reduce colorectal cancer risk. However, surveillance interval documentation practices are highly variable for clinicians and may impact effective communication of timing of repeat colonoscopy. The aim of our study was to characterize the documentation practices for surveillance intervals among gastroenterologists within a large, academic health center. Click here for full abstract
Documentation practices of withdrawal time and bowel preparation quality in screening colonoscopy reports in a large academic health center
Robert Tamai, MD; Folasade P. May, MD, PhD, MPhil
Introduction: Appropriate documentation of colonoscopy quality indicators is critical to assess and monitor colonoscopy quality assurance. However, comprehensive documentation is time-consuming, burdensome, and highly variable among clinicians. This variation hinders efforts to accurately capture, measure, and track colonoscopy quality. The aim of our study was to characterize the screening colonoscopy documentations practices for withdrawal time and bowel preparation quality among gastroenterologists within a large, academic health center. Click here for full abstract
Evaluating the performance of an EHR-based clinical dashboard to track follow-up colonoscopy for abnormal FIT
Helen Xu, MD; Bita Shahrvini, MD; Nicholas Valle, MD; Vismaya Bachu, MD; Kirstin Peters, MD; Jayraan Badiee, MPH; Brandon Smith, MD; Folasade P. May, MD, PhD, MPhil
Introduction: The fecal immunochemical test (FIT) is a widely used tool for colorectal cancer (CRC) screening. Abnormal results require a follow-up colonoscopy in a two-part screening process. However, data show completion rates as low as 40-60%, likely owing to various barriers such as patient willingness to undergo a procedure, access, and linkage from primary care to gastroenterology. EHR-based clinical dashboards can be powerful tools for aggregating and tracking health system data in real-time to identify gaps in care. This study aimed to validate a feature of a CRC screening dashboard we created at our health system, which tracks colonoscopies for abnormal FIT patients. Click here for full abstract
Impact of updated colorectal cancer screening guidelines in United Stated Federally Qualified Health Centers: A cross-sectional analysis of national data
Introduction: Colorectal cancer (CRC) screening guidelines were updated May 2021 to include individuals age 45-49, owing to an observed increase in CRC incidence in young adults. The impact of this expanded eligibility on efforts to screen 80% of Americans, particularly in communities already facing notable barriers to screening, is poorly understood. Our study investigates the impact of including this new age group on CRC screening rates at all United States (US) Federally Qualified Health Centers (FQHCs). Click here for full abstract
Implementing linguistically tailored colorectal cancer risk assessment in a multi-site pragmatic clinical trial to improve screening in community health centers
Nicolette J. Rodriguez, MD, MPH; Chinedu Ukaegbu, MBBS, MPH; Susan Regan, PhD; Jessica J. Tuan, MPH; Suzanne Brodney, PhD, MS; Beth Glenn, PhD; Yixuan Zhou; Adjoa Anyane-Yeboa, MD, MPH; Caylin Marotta, MPH; Andrew T. Chan, MD, MPH; Catherine Jeffries; Kelley Le Beaux, MA; Samantha Kuney, MA; Kimberly Schoolcraft; Anjelica Q. Davis, MPPA; Erica T. Warner, ScD, MPH; Beverly Moy, MD, MPH; David A. Drew, PhD; Gina Johnson; Yuchiao Chang, PhD; Jennifer S. Haas, MD, MSc; Folasade P. May, MD, PhD, MPhil; Sapna Syngal, MD, MPH
Introduction: Colorectal cancer (CRC) incidence and mortality disproportionately affect minority racial/ethnic groups. These groups are less likely than White populations to receive appropriate risk assessment, cancer screening and genetic testing. We describe the development and implementation of a CRC risk assessment tool in the Community Collaboration to Advance Racial/Ethnic Equity in Colorectal Cancer Screening (CARES) trial to assess appropriateness of stool based screening and ensure follow-up after abnormal screening test results. Click here for full abstract
Real-world clinical outcomes of blood-based colorectal cancer screening: Updated findings on colonoscopic follow-up
Timothy A. Zaki, MD; Nicole J. Zhang, MPH; Victoria M. Raymond, MS; Nick Ioannou, MD, PhD, MHA; Shaun P. Forbes, PhD; Amar K. Das, MD, PhD; Folasade P. May, MD, PhD, MPhil
Introduction: Blood-based tests for colorectal cancer (CRC) are emerging as convenient, non-invasive screening options with potential to improve screening participation and outcomes. Like all non-colonoscopic screening tests, blood-based screening is a two-step process in which individuals with an abnormal result must undergo follow-up colonoscopy (FU-CY). It is unclear if individuals who select blood-based screening are likely to complete this critical second step. To gain insight, we analyzed real-world closed claims data to determine the FU-CY rate after an abnormal blood-based test result and identify predictors of FU-CY. Click here for full abstract
Sociodemographic disparities in survival from localized versus metastatic gastric cancer: A SEER-based analysis
Sigrid S. Young, MD; Jayraan Badiee, MPH: Folasade P. May, MD, PhD, MPhil
Introduction: Despite decreasing incidence, gastric cancer (GC) remains the 4th leading cause of cancer-related deaths worldwide. In the United States (US), routine endoscopic screening for GC in average-risk individuals is not recommended, and most patients present with advanced disease. Five-year survival for GC decreases from 75% in localized disease to 7% in distant metastatic disease. We aimed to determine sociodemographic differences in survival rates in localized vs. metastatic GC. Click here for full abstract
Use of a large language model to ad with clinical trial recruitment for patients with non-advanced colorectal polyps
Jamie Yang, MD, Alicia Maehara; Cleo Maehara, MD, MMSC; Alexandria Uy; Odet Kachikian, MHA; Gordon Guyant; Melissa Saul; Jeffrey M. Dueker, MD, MPH; William Hsu, PhD; Folasade P. May, MD, PhD, MPhil; Robert E. Schoen, MD, MPH
Introduction: The optimal surveillance colonoscopy guideline for patients with 1 or 2 non-advanced colorectal adenomas is uncertain. FORTE1 is a national, multicenter clinical trial randomizing participants with 1 or 2 non-advanced adenomas to surveillance colonoscopy at 5 and 10 years versus 10 years. However, clinical trial recruitment is often challenging, as manually identifying eligible participants requires review of large volumes of colonoscopy, pathology, and clinical reports—a process that is resource-intensive and time-consuming, which can hinder trial efficiency. To address this challenge, we developed and evaluated a customized large language model (LLM) that uses artificial intelligence to streamline the identification of potentially eligible trial participants. Click here for full abstract
DDW Abstracts 2024
A Comparison of Four Population Health System Approaches to Increase Colorectal Cancer Screening in Young Adults
Rebecca Ekeanyanwu, MHS; Brandon C. Smith, MD; Artin Galoosian MD, MA; Jayraan Badiee, MPH; Sitaram Vangala, MS; Sadie De Silva MD; Folasade P. May MD, PhD, MPhil
Introduction: To identify effective population health approaches to increase colorectal cancer (CRC) screening participation in individuals age 45 to 49, our health system implemented and compared four screening outreach strategies. In this secondary analysis, we compared the effectiveness of each strategy by race/ethnicity to inform future screening outreach in our health system, address screening disparities, and improve the overall screening rate. Click here for full abstract
Colorectal Cancer Screening Rates Continue to Fall Behind in Federally Qualified Health Centers Serving Majority Hispanic or Majority Black Patients
Matthew Y. Zhao, BS; Vidhi Singh, BS; Megan M. Aaronson, MD, MS; Sadie R. De Silva, MD; Hayraan Badiee, MPH; Folasade P. May, MD, PhD, MPhil
Introduction: National data suggest that racial and ethnic disparities in colorectal cancer (CRC) screening are decreasing, reflecting success of equity-driven initiatives across the United States. However, there is a paucity of data on CRC screening trends in low-income and underinsured populations such as those at Federally Qualified Health Centers (FQHCs). To evaluate national progress towards equity in this setting, we assessed FQHC CRC screening rates by race/ethnicity. Click here for full abstract
Early Implementation Results from a Population Health Intervention to Close Colorectal Cancer Screening Gaps Using an Electronic Patient Decision Aid
Sadie De Silva, MD; Brandon C. Smith, MD; Sarah Meshkat, MHA; Laurie Smith, MHA, MBA; Christopher Saigal, MD, MPH; Anna Dermenchyan, PhD, RN; Hisae Suekane; Chad Villaflores, BS; Jayraan Badiee, MPH; Folasade P. May, MD, PhD, MPhil
Introduction: Population health interventions are needed to increase colorectal cancer (CRC) screening participation. WiserCare is an electronic-based patient decision aid ordered by primary care providers (PCPs) that assesses patient preference and provides individualized risk anaylysis and options for CRC screening modalities. This study is a preliminary analysis of process measures related to the implementation of WiserCare in an academic health center. Click here for full abstract
Evaluating Performance of an Artificial Intelligence Tool to Identify Individuals in Need of Three-Year Colorectal Cancer Post-Polypectomy Surveillance
Jaime Yang, MD; Sadie De Silva, MD; Brandon C. Smith, MD; Camille Soroudi, MD; Anthony Myint, MD; Bita Shahrvini, MD; William Hsu, MD; Cleo Maehara, MD; Jayraan Badiee, MPH; Alexandria Uy; Yuna Kang, MD; Bita Naini, MD; Ventakaraman Muthusamy, MD, MS; Eric Esrailian, MD, MPH; Folasade P. May, MD, PhD, MPhil
Introduction: Post-polypectomy surveillance aims to increase early detection and prevention of colorectal cancer (CRC). High risk neoplasia (HRN), defined as adenoma or sessile serrated polyp (SSP) greater than 1 centimeter, adenoma with tubulovillous or villous histology, highgrade dysplasia, >5 adenomas or SSPs, or traditional serrated adenoma, increase CRC risk and require a 3-year surveillance interval as per the 2020 United States Muti-Society Task Force (MSTF) guidelines. We previously developed and implemented a natural language processing (NLP) algorithm that uses artificial intelligence (AI) to extract data from colonoscopy and pathology reports to determine guideline-concordant surveillance intervals. In this study, we aimed to evaluate the NLP’s false negative rate for 3-year surveillance to help assess its overall performance before broad application in a health system intervention. Click here for full abstract
Feasibility of a Colorectal Cancer Screening Decision Aid Delivered Via the Patient Portal to Increase Screening Participation in a Large Academic Health Center
Brandon C. Smith, MD; Sadie De Silva, MD; Laurie Smith, MPH, MBA; Anna Dermenchyan, PhD, RN; Hisae Suekane; Chad Villaflores, BS; Jayraan Badiee, MPH; Christopher Saigal, MD, MPH; Folasade P. May, MD, PhD, MPhil
Introduction: There are several recommended colorectal cancer (CRC) screening modalities, and patient preference is contingent on factors such as eligibility, invasiveness, time required, and effectiveness. Patients who select a modality aligned with their preferences are more likely to complete screening. We aimed to assess the feasibility of an electronic decision aid to increase CRC screening participation and to inform implementation of a future large-scale decision aid intervention. Click here for full abstract
Improving Rates of Pre-Procedural Diagnostic Workup Before Anti-Reflux Procedures
Anthony Myint, MD; Sonia Divakaran, RN-BC; Jayraan Badi, MPH; Folasade P. May, MD, PhD, MPhil; Kevin Ghassemi, MD
Introduction: Anti-reflux procedures provide an important treatment option for patients with medically refractory gastroesophageal reflux disease (GERD) but are dependent on proper patient selection through pre-procedural testing. We assessed the rates of pre-procedural test completion for patients who completed an anti-reflux procedure in a large academic health system and to determine factors associated with incomplete preprocedural testing. Click here for full abstract
New Screening Tests, Same Challenge: An Early Look at Colonoscopic Follow-up After Abnormal Blood-Based Colorectal Cancer Screening Results in a Real-World Setting
Timothy A. Zaki, MD; Nicole J. Zhang, MPH; Victoria M. Raymond, MS; Nick Ioannou, MD, PhD, MHA; Shaun P. Forbes, PhD; Amar K. Das, MD, PhD; Folasade P. May, MD, PhD, MPhil
Introduction: Blood-based screening tests for colorectal cancer (CRC) are becoming increasingly prevalent and have the potential to improve adherence with screening guidelines and overall CRC outcomes. As for all non-colonoscopic screening tests, abnormal blood-based test results require follow-up colonoscopy (FU-CY) to complete the screening process. We aimed to perform one of the first analyses of FU-CY rates after abnormal blood-based screening test results and determine predictors of follow-up. Click here for full abstract
Perception of Personal and Health System Adenoma Detection Rates are Variable Among Practicing Gastroenterologists
Sadie De Silva, MD; Marc Kaneshiro, MD; Brandon C. Smith, MD; Jamie Olivia Yang, MD; Michael Bethlehem; Cleo K. Maehara; Alexandria Uy; William Hsu, MD; Jayraan Badiee, MPH; Folasade P. May, MD, PhD, MPhil
Introduction: Adenoma detection rate (ADR) is correlated with low risk of interval colorectal cancer (CRC) and reflects the overall effectiveness of screening colonoscopy. Accurate provider perception of performance can enhance quality efforts while inaccurate perception can hinder progress. We aimed to examine the perception of gastroenterologists (GIs) on ADR in a large academic health system. Click here for full abstract
Rurality of Residence and Disparity in Incident Hepatocellular Carcinoma
Nguyen V. Pham; Mei Leng; Steven-THuy Han, MD; Folasade P. May, MD, PhD, MPhil; Jihane N, Benhammou, MD, PhD
Introduction: Hepatocellular carcinoma (HCC) is increasing in prevalence among Veterans. We have shown that Vietnam Veterans who self-identified as Hispanic and non-Hispanic Black were more likely to develop HCC, compared to non-Hispanic White Veterans. Identifying clinical and social determinants of health (SDOH) associated with HCC disparities has the potential to improve detection and treatment of HCC in vulnerable Veterans. Click here for full abstract
To Screen or Not to Screen: Why Young People Choose to Participate in Colorectal Cancer Screening
Rebecca Ekeanyanwu, MHS; Jayraan Badiee, MPH; Sitaram Vangala, MS; Brandon C. Smith, MD; Artin Galoosian MD, MA; Folasade P. May MD, PhD, MPhil
Introduction: In 2022, our health system conducted a randomized controlled trial to compare four screening outreach approaches for average-risk individuals age 45 to 49. In this follow-up survey, we aimed to determine the factors that influence decision-making and screening practices of young adults at average-risk for CRC and newly eligible for screening. Click here for full abstract
Use of Health Information Technologies in Federally Qualified Centers Predicts High Colorectal Cancer Rates
Vidhi Singh, MD; Matthew Y. Zhao, BS; Megan A. Aaronson, MD, MS; Jayraan Badiee, MPH; Folasade P. May MD, PhD, MPhil
Introduction: Federally Qualified Health Centers (FQHC) offer preventive health services, including colorectal cancer (CRC) screening, to low-income and under-insured individuals in the United States (U.S.). Some FQHCs utilize health information technologies (HIT) such as kiosks, patient portals, and automated preventive care outreach to improve patient engagement and collect social risk factor (SRF) data. We aimed to determine the relationship between the use of HIT for this purpose and CRC screening rates in FQHCs. Click here for full abstract
Variation in Baseline Colorectal Cancer Screening Rates and Modalities in a Multi-Region Trial in Community Health Centers
Jessica J. Tuan, MPH; Adjoa Anyane-Yeboa MD MPH; Erica T. Warner, ScD, MPH; Yixuan Zhou; Suzanne Brodney, PhD, MS; Andrew T. Chan, MD, MPH; David A. Drew, PhD; Beth Glenn, PhD; Ellen T. Lee, BS; Nicolette J. Rodriguez, MD, MPH; Kimberly Schoolcraft; Sapna Syngal, MD, MPH; Jennifer S. Haas, MD MSc; Folasade P. May, MD, PhD, MPhil
Introduction: Colorectal cancer (CRC) screening is underutilized, especially in community health centers (CHCs) that provide primary care services to low-income, uninsured, and racial/ethnic minority populations. The Community Collaboration to Advance Racial/Ethnic Equity in CRC Screening (CARES) study aims to increase CRC screening rates in CHCs in three regions of the United States. In this pre-intervention analysis, we aimed to evaluate baseline CRC screening rates and CHC characteristics in FQHCs in two of the study regions. Click here for full abstract
Younger Age and Self-Reported Anxiety about Paying Medical Bills are Associated with Decreased Odds of Flu Vaccination in Patients with Inflammatory Bowel Disease
Amarachi Erondu, MD; Folasade P. May, MD, PhD, MPhil; Jenny S. Sauk, MD; Nirupama N. Bonthala, MD; Berkeley N. Limketkai, MD, PhD
Introduction: Patients with inflammatory bowel disease (IBD) have an increased risk of contracting infections that are preventable by vaccines. According to clinical guidelines, patients with IBD should receive the flu vaccination yearly. In this study, we used nationwide data from the United States National Health Interview Survey to determine demographic and socio-economic factors associated with flu vaccination in patients with IBD. Click here for full abstract